Wednesday-Friday blog
NHS worshippers’ lies
At the weekend, I used the latest Office for National Statistics figures to show that NHS England staff levels had increased by 30% to 40% in most medical and non-medical departments over the last 10 years (2013 to 2023) whereas the population of England had only increased by around 7%. So the NHS worshippers’ constant bleating that their hallowed NHS needs more staff to cope with a supposedly ‘rapidly-rising’ population is a pack of lies.
In my Monday/Tuesday blog, I used the Office for National Statistics figures to show that NHS staff levels in the three smaller parts of the UK – Scotland, Wales and Northern Ireland – had gone up by 20% to 30% in most medical and non-medical departments over the last 10 years while the population had only increased by a tiny 2.7%. More proof that the NHS worshippers’ constant bleating that their beloved NHS needs more staff to cope with a supposedly ‘rapidly-rising’ population is a pack of lies.
I also showed that Britain lies on the OECD average in the amount spent per capita on healthcare:
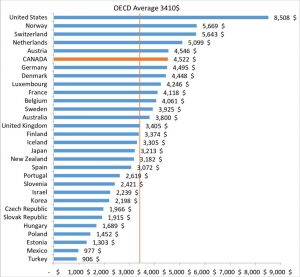
(left-click on image then left-click again to see more clearly)
This rather undermines the NHS adorers’ constant moaning that the NHS needs ever more of our money as countries where health spending per capita is less than the UK don’t appear to be permanently on the verge of collapse like our NHS.
So a rising population and a lack of spending cannot be the main reasons for our NHS’s complete failure and constant state of near collapse
The cancer disaster
I’ve just done a quick Google search on charts showing cancer survival rates by country. On all the charts I’ve seen (here are just a couple – for lung cancer and pancreatic cancer) the UK has some of the lowest cancer survival rates for a developed country:
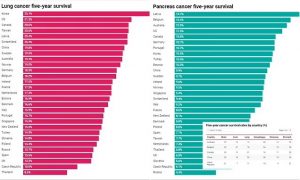
(left-click on image then left-click again to see more clearly)
And here’s a chart from The Lancet on overall cancer survival rates by country:
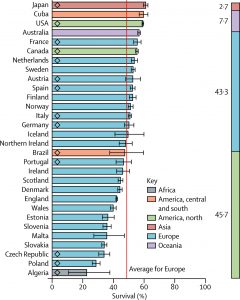
As you’ll see, England, Scotland and Wales come in worse than the European average.
I’m really begining to wonder what our million or so NHS employees actually do all day. I suspect that due to incompetent management and a general ‘nobody gives a damn’ attitude there are vast amounts of waste – operating theatres are idle most of the time, expensive kit like MRI scanners are underutilised, patient files and blood test results are constantly getting lost, tens of thousands of hours of frontline staff’s time are wasted on garbage like ultra-woke critial race theory and diversity training, an increase in ethnic diversity has led to a huge increase in corruption and billions are lost through finanical mismanagement and appalling purchasing.
When I was very briefly an elected governor for my local hospital, I tried to raise the issue that a whistleblower had claimed to me that the hospital had been cheated out of over £1m due to overcharging (using what’s called ‘cover pricing’) by the construction company which built the hospital’s £5m+ multi-storey car park. Cover pricing (also known as cover bidding) is a common form of bid-rigging scheme. It is used during a competitive tender process as a way of fixing a bid to give an unfair advantage to a specific bidder. The objective is to give the appearance of genuine competition, when in reality the bids are not competing. Hospital management informed me in no uncertain terms that hospital internal management matters were none of my business and, when I had a meeting with the NHS’s own corruption investigators, they refused to look into the matter.
My proposition therefore is: The real cancer killing us is the uselessness of our failing NHS full of arrogant, lazy, incompetent but ethnically- and gender-diverse staff and worthless over-paid, over-pensioned, self-serving and in some cases corrupt bureaucrats.








It would be interesting to see the survival rates for private hospitals. Would it be better and would it be enough to make people give up their holidays and entertainment to pay for private care?
Problem with private hospital care, Thorpe, is that few, if any, private hospitals have Intensive Care Units, meaning that although a patient may pay, say £15,000 for a hip replacement, if that patient suffers a life-threatening event during the procedure or post-operatively, a condition requiring Intensive Care, he or she will be conveyed at maximum speed to the nearest NHS Intensive Care unit, where there is all the essential equipment, in order to receive round-the-clock care by the NHS ITU team. In all my years interacting with NHS patients, I never ceased to be astonished that almost all those opting for private surgery looked no further when making that choice than the fact that they would have a private room and that the food would be better. Having said that, I certainly do agree that the NHS is now sinking under the weight of its own bureaucracy, which regularly fails to update such elementary but essential patient information such as current address. Not to mention the millions being splashed on idiotic woke staff positions.
I agree about Private hospitals. There is a lot they do not do, but that is because they can fall back on the NHS. My point was to ask whether people would be prepared for an improved service if available. I suspect not which is why there will be no improvement. Private hospitals are unable to deal with some emergency conditions if they arise and have to transfer patients to the NHS, which means additional risks. I don’t know whether they inform patients about this. I suspect that they will also refuse to treat patients if there is a high risk associated with the operation.
I know of somebody who arranged a hip replacement in Brighton and lived in Eastbourne and when she arrived her they had forgotten to tell her to stop her blood thinning medication so it could not be done at that time. There was also no physiotherapy included and she had to arrange that separately.
Overall between NHS and private it is completely unsatisfactory and in my view it is because the NHS dominates.